CLINICAL TAKEAWAY | Domain | Key Finding | Evidence Level | | CV Mortality | ~14% all-cause mortality reduction; ~21% relative reduction in major vascular events per 1 mmol/L LDL lowered | Strong (RCT meta-analysis) | | Side Effects | 90% of symptom burden is nocebo; no difference between statin and placebo in blinded crossover (SAMSON) | Strong (NEJM, n-of-1 RCT) | | Cancer Risk | RCTs show no effect on cancer incidence; observational data suggests site-specific reductions (liver, colorectal). Signal is hypothesis-generating, not confirmed. | Weak–Moderate (conflicting) | | Dementia / AD | New RWD analysis (Novak 2026, n=838K PSM): RR=0.69 for AD. Cochrane RCTs (n=26K) remain negative for late-life initiation. Signal is accumulating — causality unproven. | Conflicted — RWD signal strengthening; RCT data negative for late life | | Cost | All major statins are generic; widely available for <$10/month, often covered with $0 copay | Established fact |
| |
|
Every morning I open the same orange bottle, tap out a small white pill, and swallow it without ceremony. I'm 36. I have no symptoms. I haven't had a heart attack. My cardiologist hasn't referred me anywhere. I started this four years ago — not out of fear, but out of an honest accounting of the evidence. |
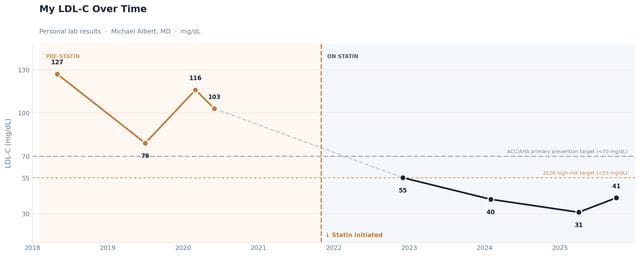
My LDL in May 2018 was 127 mg/dL. I was 28 years old, apparently healthy, and no one in the room was particularly alarmed. By conventional thresholds, they shouldn't have been. But it wasn't where it needed to be — and, more importantly, I knew that the relevant question wasn't where I was at 28, but where my vascular biology would be at 60 if I didn't act. |
Over the next two years my LDL fluctuated between 79 and 127 mg/dL — the kind of variation that looks unremarkable on a single visit, more meaningful over a trend. I started a statin in late 2021. My most recent value: 31 mg/dL. |
|
As a physician, I've spent years counseling patients about statins. I've watched people stop them over muscle aches that turned out to be entirely independent of the drug. I've watched people avoid them because they feared dementia — a fear the RCT data has consistently failed to confirm. And I've watched cardiovascular events happen to people who, by all algorithmic logic, should have been on one. |
Eventually, it felt disingenuous not to apply the same reasoning to myself. |
What follows is my honest read of the evidence: what statins actually do in primary prevention, what they don't do, and why I think the risk-benefit calculation for a large portion of middle-aged adults has become, quietly, one of the clearest in all of preventive medicine. |
The Case for Primary Prevention |
The foundational data on statins for primary prevention comes from the Cholesterol Treatment Trialists' (CTT) Collaboration — the most comprehensive individual patient-level meta-analysis of statin therapy ever assembled. Across 27 randomized trials involving more than 170,000 participants, the CTT found that each 1 mmol/L (roughly 38.7 mg/dL) reduction in LDL cholesterol produced approximately a 21% relative reduction in major vascular events — heart attacks, strokes, and coronary revascularizations — regardless of baseline cardiovascular risk. |
Crucially, this benefit was observed even in people at lower risk — people like me. The 2012 CTT analysis specifically examined individuals with a 5-year risk of major vascular events below 10%, and found approximately 11 fewer major vascular events per 1,000 people treated over 5 years per mmol/L of LDL lowered. That benefit, they argued, substantially exceeded any known harm from statin therapy. |
A Cochrane systematic review of statins for primary prevention synthesized 18 randomized controlled trials and found a statistically significant reduction in all-cause mortality (OR 0.86, 95% CI 0.79–0.94). Fatal and non-fatal cardiovascular events, coronary heart disease events, and strokes were all meaningfully reduced. The review also found no evidence of serious harm. |
KEY DATA · CTT COLLABORATION 21% Relative risk reduction in major vascular events per 1 mmol/L LDL lowered | 14% All-cause mortality reduction in primary prevention (Cochrane review) | 170K+ Participants in the CTT individual patient data meta-analyses |
|
|
Critics — and there are legitimate ones — point out that the absolute risk reductions in primary prevention are modest, particularly over short follow-up periods. A meta-analysis by Byrne and colleagues in JAMA Internal Medicine found absolute risk reductions of 0.8% for all-cause mortality and 1.3% for MI over the study period. That's real, but it's not dramatic. I think that framing misses something important: atherosclerosis doesn't wait for you to notice it, and cardiovascular risk compounds over decades. The question for a 36-year-old isn't "will this help me in the next five years?" It's "what does my vascular biology look like at 60 if I start now versus if I wait?" |
Mendelian randomization studies — which use genetic variants as proxies for lifelong LDL exposure — suggest the cardiovascular benefit of lower LDL is substantially larger when it begins early in life. The biology of plaque formation is cumulative. Starting at 36 is not the same as starting at 60. |
What the Individual Trials Actually Show |
The meta-analytic consensus rests on a foundation of landmark individual trials worth naming, because the denialism movement has a habit of cherry-picking the negative ones. |
WOSCOPS — the first major primary prevention RCT — enrolled over 6,500 men with elevated LDL and found a 3.3% absolute reduction in all-cause mortality with pravastatin (HR 0.88, 95% CI 0.79–0.99, p=0.03) over 20 years of follow-up. JUPITER randomized 17,800 apparently healthy adults with elevated hs-CRP and normal LDL to rosuvastatin vs. placebo; all-cause mortality fell significantly (HR 0.80, 95% CI 0.67–0.97, p=0.02). MEGA, conducted in a Japanese primary prevention population, found coronary heart disease events reduced by 33% with pravastatin (HR 0.67, p=0.01). HOPE-3 extended the benefit to an ethnically diverse intermediate-risk population with no prior CVD: rosuvastatin reduced the primary CV composite (CV death/MI/stroke) by 24% (HR 0.76, 95% CI 0.64–0.91; p=0.002). All-cause mortality was not significantly reduced in the 5.6-year trial. And PROSPER, in a mixed primary/secondary prevention population of older adults (age 70–82), showed coronary disease mortality fall by 24% (p=0.043). |
There are also negative trials. ALLHAT-LLT found no all-cause mortality benefit for pravastatin over usual care (RR 0.99, p=0.88). That result matters and shouldn't be dismissed. But it is one trial — with methodological limitations including substantial cross-contamination between arms — against a robust meta-analytic signal from the CTT and Cochrane reviews. Individual trial heterogeneity is expected; that is precisely why we meta-analyze. |
THE "LOWER FOR LONGER" PRINCIPLE LDL reduction compounds over time, not just over milligrams. Mendelian randomization studies of genetic variants associated with lifelong lower LDL demonstrate roughly three times the proportional risk reduction per mmol/L compared to statin trials that begin in mid-to-late life — because the exposure window is decades longer. Five years of therapy: ~22% risk reduction. Forty years: ~54%. This is why short-term absolute risk reductions in primary prevention trials — which critics correctly point out are modest — are almost certainly underestimates of the lifetime benefit of starting at 36. Every untreated year is accumulating atherosclerotic burden that doesn't announce itself until it does. I covered this in depth in the LDL article → |
|
|
The Numbers, With My Name on Them |
I debated whether to include this. But it felt dishonest not to — the whole premise of this article is physician vulnerability paired with clinical reasoning, and nothing is more concrete than actual lab work. |
These are my actual lipid results, from 2018 to late 2025. Not anonymized population data from a trial in Perth. My labwork, from an outpatient portal in Oklahoma. |
LDL-C VALUES FROM PERSONAL LAB RECORDS · ALL DATA POINTS REPRESENT FASTING LIPID PANELS | Date | LDL-C | Status | | May 2018 | 127 mg/dL | Pre-statin | | Jul 2019 | 79 mg/dL | Pre-statin | | Mar 2020 | 116 mg/dL | Pre-statin | | Jun 2020 | 103 mg/dL | Pre-statin | | Dec 2022 | 55 mg/dL | On statin · first check | | Feb 2024 | 40 mg/dL | On statin | | Apr 2025 | 31 mg/dL | On statin + ezetimibe · lowest recorded | | Oct 2025 | 41 mg/dL | On statin + ezetimibe · most recent |
| |
|
The pre-statin picture is instructive. My peak LDL was 127 mg/dL in May 2018 — "borderline" by the old framework that used 130 as the alarm threshold, unremarkable by the cultural standard of "you seem healthy." The 79 in mid-2019 was a motivated, vegetable-heavy stretch I couldn't sustain; by spring of 2020 it was back to 116. This is the natural history of diet-only LDL management in most people: transient, unstable, incomplete. |
What the chart shows on the right side of that dividing line is not subtle. At my first post-statin check in December 2022: LDL 55 mg/dL — already below the 2026 ACC/AHA primary prevention target of 70. My most recent value is 41 mg/dL. My total cholesterol is currently 94. For reference, 94 is lower than the average American's LDL-C alone. |
Full disclosure requires one more data point: I added ezetimibe 10 mg in November 2024. Ezetimibe works through a different mechanism than statins — it blocks intestinal cholesterol absorption rather than hepatic synthesis — and the IMPROVE-IT trial demonstrated that adding it to statin therapy reduced cardiovascular events further in high-risk patients. It is now generic and inexpensive. The lower values in the table — 31 and 41 mg/dL — reflect statin plus ezetimibe, not statin alone. I mention this not to complicate the argument, but because the premise of this article is transparency. The decision-making logic is the same: evaluate the evidence, accept a small daily inconvenience, act before the symptom announces itself. |
MY NUMBERS · 2018–2025 127 → 41 LDL peak → most recent value (mg/dL). A 68% reduction. | 31 mg/dL Lowest recorded LDL (Apr 2025) — in the range of PCSK9 loss-of-function carriers | 94 mg/dL Current total cholesterol — lower than the average American's LDL-C alone (~116 mg/dL) |
|
|
I want to be careful not to turn personal lab data into a performance. The LDL number is not the point. The point is that I spent several years in the 100–127 range — well below the old "treat" threshold of 190, technically "normal" on most lab printouts — while atherosclerosis runs on a different accounting system than the reference range at the bottom of the page. Plaque doesn't wait for the alert flag. |
I am now accumulating years at an LDL in the 31–55 range, starting in my mid-30s. If the Mendelian randomization literature is directionally right, that compounding will look very different at 65 than it would have on the trajectory I was on. That is not certainty. It is a reasonable bet on a low-cost, well-tolerated intervention with a 30-year evidentiary foundation. |
The Side Effect Problem We Invented |
Here is one of the most important and underappreciated facts in all of outpatient medicine: more than half of patients who start a statin abandon it within two years. The most commonly cited reason is side effects, predominantly myalgia — muscle pain. And yet, in blinded, placebo-controlled trials involving more than 80,000 participants, there is no excess in symptomatic side effects in patients taking statins compared to those taking placebo. |
This paradox — real symptoms, no pharmacological signal — was elegantly resolved by the SAMSON trial, published in the New England Journal of Medicine in 2020. Sixty patients who had previously discontinued statins due to intolerable side effects were enrolled in an n-of-1, double-blind, crossover trial. Each participant received 12 one-month medication bottles — four containing atorvastatin 20 mg, four containing placebo, and four empty — in a randomized sequence. They reported daily symptom severity on a smartphone app. |
SAMSON TRIAL · NEJM 2020 8.0 Mean symptom score (0–100 scale) during no-tablet months | 15.4 vs 16.3 Placebo vs Statin months — statistically indistinguishable (P=0.39) | 90% Calculated nocebo ratio — 9 in 10 symptoms attributable to taking the tablet, not the statin |
|
|
The result was striking. Symptom scores were nearly identical during placebo and statin months — both significantly higher than no-tablet months. The calculated nocebo ratio was 0.90: ninety percent of the statin-attributed symptom burden was equally present on placebo. The act of taking a tablet — not the molecule inside — was driving the experience. |
The clinical implication is profound: when patients are told these findings directly, half of them successfully restart statin therapy. The symptoms are real. The cause is not the statin. This is not gaslighting patients — it is giving them genuinely useful, empowering information. |
I have shared SAMSON with dozens of patients in my practice over the past few years. It is one of the most practically useful single pieces of evidence I keep in my clinical toolkit. I have watched people who'd given up on statins revisit the decision with completely different framing — and stay on therapy. |
The Cancer Question: Promising Signals, Honest Caveats |
This is where I'll ask you to hold two things simultaneously: a biologically plausible hypothesis and an honest accounting of what the randomized trial data actually shows. |
The hypothesis is this: statins inhibit the mevalonate pathway, disrupting cholesterol synthesis in ways that may interfere with cancer cell proliferation, angiogenesis, and metastasis. Rapidly dividing cells — the hallmark of cancer — require more cholesterol for membrane synthesis. Statins also reduce prenylation of proteins like Ras and RhoA GTPases, altering downstream signaling in ways that can promote apoptosis and suppress tumor growth. This is real, well-characterized biology. |
The observational literature is genuinely intriguing. An umbrella meta-analysis of 71 meta-analyses across 14 cancer sites found that statin use was associated with reduced likelihood of biliary tract cancer (33%), liver cancer (42%), gastric cancer (29%), colorectal cancer (9%), and several hematologic malignancies. These are not trivial numbers in isolation. |
⚠ EXTRAPOLATION — INTERPRET WITH CAUTION The cancer hypothesis is speculative for primary prevention. The CTT Collaboration's analysis of individual patient data from 175,000 participants across 27 statin trials found no effect of statin therapy on overall cancer incidence (RR per 1 mmol/L LDL reduction = 1.00, 95% CI 0.96–1.04), and no increase in cancer mortality at any of 23 individual cancer sites. A 2023 meta-analysis of 35 RCTs similarly found no reduction in cancer incidence (OR 0.99, 95% CI 0.95–1.03) or cancer mortality. The observational benefit signals are likely confounded by indication, healthy user bias, and survivorship effects. I do not take a statin for cancer prevention. Neither should you — not yet, on current evidence. But the biology keeps the question interesting. |
|
The Dementia Question: More Complicated Than It Was |
Dementia fear is real, and it's frequently invoked as a reason to either take or avoid statins — depending on who's talking. The evidence here has evolved meaningfully in the past year, and it deserves an honest accounting. |
The foundational tension: observational studies consistently show statin users have lower dementia and Alzheimer's risk — a 2022 meta-analysis of 46 studies and over 7 million patients found a 20% reduction in all-cause dementia and a 32% reduction in Alzheimer's disease. Striking numbers, but plagued by the healthy user effect. Two large RCTs (Cochrane 2016, n=26,340) remain negative — statins given in late life to people at vascular risk do not prevent cognitive decline or dementia in trial conditions. |
In 2026, a new entry into this debate: Novak et al. published a real-world data analysis using the TriNetX federated EHR network — over 125 million U.S. patients — and applied rigorous propensity score matching on 838,000 statin users and 838,000 matched non-users with dyslipidemia and no prior Alzheimer's diagnosis. They excluded diabetes, prior cerebrovascular disease, and known dementia confounders, and used a new-user design to minimize immortal time bias. |
|